


Are We Entering the Era of Personalized Osteotomy Surgery?
Theodore Shybut, M.D., FAANA
Member AANA Communications and Technology Committee
Osteotomies about the knee – including high tibial osteotomy (HTO), distal femoral osteotomy (DFO) and tibial tubercle osteotomy (TTO) – remain powerful joint preservation tools for managing malalignment, instability and focal cartilage disease in young and active patients. However, these procedures can be technically demanding and are intensive in terms of surgical time and fluoroscopy exposure. These procedures require precision to optimize outcomes and carry low but significant risks of serious complications. Recent advances in advanced imaging based three-dimensional (3D) planning and patient-specific instrumentation (PSI) aim to improve accuracy, reproducibility and efficiency through personalized surgical guides and implants tailored to individual anatomy and case requirements. This article highlights the growing role of PSI in lower extremity osteotomies, focusing on HTO, DFO and TTO.
Traditional osteotomy techniques rely on two-dimensional radiographic planning and intraoperative fluoroscopic estimation to achieve desired correction. This approach is inherently limited in addressing multiplaner and complex three-dimensional deformities and may result in variability in alignment correction and tibial slope control. PSI-based techniques typically utilize standard standing long leg alignment radiographs digitally overlayed with 3D bony models obtained from computed tomography (CT) of the ankle, knee and hip. Conceptually this is similar to software utilized for robotic knee arthroplasty. The digital case plan allows for tailoring of corrections in multiple planes and is used to generate patient-specific cutting guides, with accompanying specific cutting depths, screw placements and lengths, wedge/graft dimensions for opening wedge techniques and patient-specific plates for fixation.
High tibial osteotomy is the most widely studied application of PSI for knee realignment surgery. Recent literature shows that PSI improves coronal and sagittal plane accuracy compared with conventional techniques. Deviations from planned alignment are frequently reported within 1-2°, outperforming traditional and even navigation-assisted approaches.1 A prospective comparative study demonstrated significantly smaller discrepancies between planned and achieved hip-knee-ankle (HKA) angles with PSI (0.6° vs. >2° with conventional or navigation techniques), though did not find differences in clinical outcomes or complication rates.2 A retrospective series of 23 cases found coronal plane correction accuracy of 0.8° ± 1.5°. Tibial slope change was 1.7° ± 2.2°. Postoperative CT scans with 3D reconstructions showed average rotational differences of − 0.1° ± 2.3° in coronal plane, − 0.2° ± 2.3° in transversal plane and 1.3° ± 2.1° in sagittal plane. Likewise 3D translational differences were calculated as 0.1 mm ± 1.3 mm in coronal plane, − 0.1 ± 0.6 mm in transversal plane and − 0.1 ± 0.6 mm in sagittal plane.3 Another series of 25 patients demonstrated similarly accurate coronal plane correction with mean hip knee angle difference 2.1° (SD ± 2.0°) and mean plan vs. achieved tibial slope difference 0.2° (SD ± 0.4°).4 Moreover, prospective clinical outcomes (KOOS score, EQ5D, KSS score and VAS pain scores) all significantly improved from before surgery and significantly improved over time. Recently Nguyen, et al reported similarly high accuracy in corrections and improved clinical outcomes for a series of medial opening wedge PSI-based high tibial osteotomies. Additionally they found significant medial femoral condyle articular cartilage regeneration seen at second look arthroscopies.5 In summary, the available evidence suggests PSI osteotomies achieve high accuracy and support excellent patient outcomes. There are also significant advantages in terms of resource utilization and radiation exposure for patients and surgical staff. PSI for HTO is associated with reduced fluoroscopy utilization, shorter operative time and overall streamlined case workflow.1
Distal femur osteotomy is less commonly performed compared to HTO, but the surgical principles, techniques and challenges are conceptually and mechanically similar to those of HTO. Clinical results in a series of PSI-based HTO and DFO cases include significantly improved patient-reported outcomes (IKDC, WOMAC, Lysholm), high rates of alignment within targeted correction thresholds (89% within 10 percent, median difference 3.7% which was less than 1 degree) and 91% survivorship at short to mid-term follow-up.6
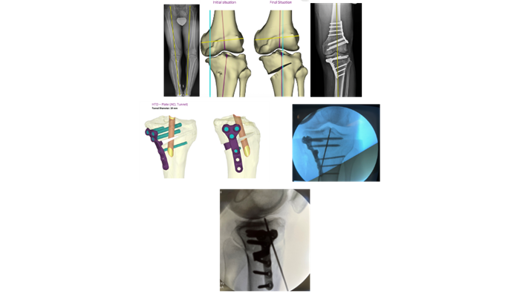
PSI can be particularly helpful in severe deformities with large corrections that are best handled with dual level osteotomy. A series of 35 of these complex cases in 31 patients demonstrated significantly improved hip-knee alignment and improved joint line obliquity, without significant difference between planned versus achieved corrections. Functional outcomes in this group were good at short to mid-term follow-up, including 100% of patients meeting MCID for improvement in WOMAC total scores.7 By way of example, in this case of a physically active individual with medial compartment post-traumatic osteoarthritis and a varus lower extremity, an opening wedge high tibial osteotomy would have resulted in a 16 mm gap at the osteotomy site. A smaller opening wedge HTO was combined with a closing wedge DFO to achieve the correction: Figure 1 shows preoperative standing alignment radiograph. Figure 2 shows preoperative plan for HTO. Figure 3 shows post-operative AP radiograph.
Likewise, 3D PSI simplifies concurrent reconstructive surgeries such as concurrent ligament reconstructions, meniscal root repair or meniscal allograft transplants, as the screw paths can be directed away from the tunnels or fixation for the soft tissue reconstructions. In addition, preoperative planning allows for custom guides to create tunnels for root repair, meniscal allograft or cruciate ligament reconstruction. For example, in this case of a chronically ACL-deficient varus knee, the preoperative plan included a guide for the ACL tibial tunnel: Figure 4 shows an image of the plan. Figure 5 shows an AP fluoroscopic image of the guide pin placed via a custom guide that overlays the custom HTO fixation implants. Figure 6 is a lateral fluoroscopic view of the same.
PSI applications for tibial tubercle osteotomy have also been developed and are now commercially available.8 While outcome data is not yet available, the potential benefits of utilizing PSI for TTO are similar to those of HTO and DFO and include: 3D modeling allows for exact modeling of multiple combinations of anteriorization, medialization, distalization and cut angle to titrate correction to case needs; PSI may improve accuracy and precision, decrease operative time and reduce fluoroscopy and potentially improve safety around complex anatomy.
Studies to date suggest the tailored approach to osteotomy that PSI allows can enhance precision, improve efficiency, reduce fluoroscopy use and radiation exposure and there are reasons to believe PSI also improves safety and ultimately optimizes outcomes. One meta-analysis found highly accurate coronal plane alignments with low rates of outliers and reduced operative time and fluoroscopy use compared to conventional techniques.9 Other studies have reported no significant outcome differences.10 Nevertheless, larger scale prospective comparative studies with longer term follow-up and sufficient power to study outcomes thoroughly remain to be done. A cadaveric study has shown that PSI based osteotomies were more accurate and resulted in reduced fluoroscopy use and radiation exposure compared to traditional techniques.11 While experienced surgeons who regularly perform these cases do not need it per se, the enhanced precision, safety, efficiency and detailed precision that 3D planning and PSI affords I think will make it essential to these cases in the very near future. I suspect surgeons like me who have performed many osteotomies both ways will overwhelmingly choose PSI. In conclusion, I believe we are indeed entering an era of personalized osteotomy surgery.
References
- Shen, M., Alaia, M. High Tibial Ostoetomy With Virtual Planning and Patient Specific Instrumentation: A Narrative Review. Annals of Joint. 2026 Jan 8:11:13. doi: 10.21037/aoj-25-44.
- Zhu, X., Qian, Y., Liu, A., Xu, P., Guo, J.J. Comparative Outcomes of Patient-Specific Instrumentation, the Conventional Method, and Navigation Assistance in Open-Wedge High Tibial Osteotomy: A Prospective Comparative Study With Two-Year Follow Up. The Knee. 2022 Dec:39:18-28. doi: 10.1016/j.knee.2022.08.013.
- Fucentese, S.F., Meier, P., Jud, L., Kochli, G., Aichmair, A., Vlachopoulos, L., Furnstahl, P. Accuracy of 3D-Planned Patient Specific Instrumentation in High Tibial Osteotomy. Journal of Experimental Orthopaedics. 2020 Feb27;7;7. doi: 1186/s40634-020-00224-y.
- Zaffagnini, S., Del Fabbro, G., Lucidi, G.A., Agostinone, P., Belvedere, C., Leadini, A., Grassi, A. Personalized Opening Wedge High Tibial Osteotomy With Patient-Specific Plates and Instrumentation Accurately Controls Coronal Correction and Posterior Slope: Results From a Prospective First Case Series. The Knee. 2023 Oct:44:89-99. doi: 10.1016/j.knee.2023.07.011.
- Nguyen TS, Gọi KY, Wong PC, Wang PY, Lin JC, Wu AF, Lin CY, Wu JL. Patient-Specific Instrumentation in Medial Proximal Tibial Angle-Based Medial Open Wedge High Tibial Osteotomy: Improved Correction, Accuracy, and Cartilage Regeneration at Second-Look Arthroscopy. Arthroscopy. Published online 10 March 2026. https://doi.org/10.1002/arj.70018
- Wang, Y., Dietrich, A., Hinz, M., Amendola, R., Dornan, G., Provencher, M., Vidal, A., Kanakamedala, A. Clinical Outcomes and Accuracy of Patient-Specific Instrumentation for Corrective High Tibial Osteotomy and Distal Femoral Osteotomy. Orthopaedic Journal of Sports Medicine. 2025 Sep 26;13(9 suppl3):2325967125S00062. doi: 1177/2325967125S00062.
- Ma, X., Zhao, Z., Bai, H., Ye, S., Zhao, B., Luo, W. Patient-Specific Cutting Guides Provide Consistent Planned Correction and Preserved Joint Line Obliquity or Double-Level Osteotomy. Arthroscopy. 2025. Nov;41(11):4713-4723. doi: 10.1016/j.arthro.2025.06.032.
- Tan, A.K., Chua, S.K., Koh, D.T., Soong, J., Rahmatullah, H., Razak, D.A., Tan, S.Y., Lee, K.H. Patient-Specific 3-Dimensional Surgical Guide For Anteriorizing Tibial Tubercle Osteotomy. Arthroscopy Techniques. 2025 Sep 25;14(12):103899. doi: 10.1016/j.eats.2025.103899.
- Arman, Z.S., DePhillipo, N.N., Peebles, L.A., Familiari, F., LaPrade, R.F., Dekker, T.J. Improved Accuracy of coronal Alignment Can Be Obtained Using 3D-Printed Patient-Specific Instrumentation For Knee Osteotomies: A Systematic Review of Level III and IV Studies. Arthroscopy. 2022 Sep;38(9):2741-2758. doi: 10.1016/j.arthro.2022.02.023.
- Pang, R., Jiang, Z., Xu, C., Shi, W., Zhang, X., Wan, X., Bahat, D., Li, H., Senatov, F., Bulygina, I., Wang, H., Zhang, H., Li, Z. Is Patient-Specific Instrumentation Accurate and Necessary For Open-Wedge High Tibial Osteotomy? A Meta-Analysis. Orthopaedic Surgery. 2023 Feb;15(2):413-422. doi: 10.1111/os.13483.
- Carey, E.G., Kamath, A.F., Vidal, A.F., Frush, T., Alaia, M., Baldwin, R.D., Ranawat, A. Assessing the Impact of Patient-Specific Instrumentation on Accuracy and Radiation Exposure in a Cadaveric Model of Medial Opening-Wedge High Tibial Osteotomy. Orthopaedic Journal of Sports Medicine. 2025 Jan 28;13(1):23259671241285430. doi: 10.1177/23259671241285430.
Interested in More Clinical Resources?
Arthroscopy Journal
- Improved Accuracy of Coronal Alignment can be Attained Using 3D-Printed Patient-Specific Instrumentation for Knee Osteotomies: A Systematic Review of Level III and IV Studies
Zachary S. Aman, B.A., Nicholas N. DePhillipo, Ph.D., A.T.C., Liam A. Peebles, B.A., Filippo Familiari, M.D., Robert F. LaPrade, M.D., Ph.D., Travis J. Dekker, M.D. - Double-Level Knee Derotational Osteotomy Yields Better Postoperative Outcomes Than Tibial Tubercle Transfer Combined with Medial Patellofemoral Ligament Reconstruction in Patients with Recurrent Patellar Instability and Severe Malrotation
Yi Qiao, M.D., Xiulin Wu, M.D., Jinlong Wu, M.D., Simin Lu, M.D., Song Zhao, M.D., Jinzhong Zhao, M.D. - Editorial Commentary: Is High Tibial Osteotomy All We Need? No Differences in Patient-Reported Outcomes in Medial Meniscal Posterior Root Tears with Varus Deformity Between Isolated High Tibial Osteotomy and Osteotomy with Meniscal Centralization and All-Inside Root Repair
Andrew S. Bi, M.D. - Patient-Specific Cutting Guides Provide Consistent Planned Correction and Preserved Joint Line Obliquity for Double-Level Knee Osteotomy
Xinlong Ma, M.D., Zhihu Zhao, M.D., Haohao Bai, M.D., Songqing Ye, M.D., Bin Zhao, M.D., Wei Luo, M.D.
Arthroscopy Techniques
- Patient-Specific 3-Dimensional Surgical Guide for Anteriorizing Tibial Tubercle Osteotomy to Treat Patellofemoral Osteoarthritis
Ashton Kai Shun Tan, M.B.B.S., Shaun Kai Kiat Chua, M.B.B.S., M.R.C.S., Don Thong Siang Koh, M.B.B.S., M.R.C.S., Junwei Soong, M.B.B.S., M.R.C.S., F.R.C.S., Hamid Rahmatullah Bin Abd Razak, M.B.B.S., G.D.F.M., M.R.C.S., M.F.S.T., F.R.C.S., F.A.M.S., M.P.H., Shing Yi Tan, Kong Kwee Lee, M.B.B.S., M.R.C.S., F.R.C.S. - Combined Medial Opening-Wedge High Tibial Osteotomy and Revision Medial Meniscus Posterior Root Repair Using a Transtibial Double-Tunnel Pullout Technique
Evan P. Shoemaker, B.A., Luke V. Tollefson B.S., Matthew T. Rasmussen, M.D., Dustin R. Lee, M.D., Robert F. LaPrade, M.D., Ph.D.
Arthroscopy, Sports Medicine and Rehabilitation
- Knee Osteotomies can be Performed Safely in an Ambulatory Setting
Michael Doran, M.D., Anthony A. Essilfie, M.D., Eoghan T. Hurley, M.D., Ph.D., David A. Bloom, M.D., Amit K. Manjunath, M.D., Laith M. Jazrawi, M.D., Eric J. Strauss, M.D., Michael J. Alaia, M.D. - Combined Medial Patellofemoral Ligament Reconstruction and Tibial Tubercle Osteotomy has a Lower Risk of Recurrent Instability Requiring Revision Stabilization at 2 Years Than Either Procedure Alone
Alexander R. Markes, M.D., Ramesh B. Ghanta, M.D., Alan L. Zhang, M.D., C. Benjamin Ma, M.D., Brian T. Feeley, M.D., Drew A. Lansdown, M.D. - Tibial Tubercle Osteotomies Performed in an Outpatient Setting have a Low Rate of Early Complications
Thomas E. Moran, M.D., Adam J. Tagliero, M.D., Richard E. Campbell, M.D., G. Bradley Reahl, M.D., Elizabeth K. Driskill, B.S., Alexander J. Wahl, B.S., David R. Diduch, M.D. - The Ability to Achieve a Specific Target Angle on Weightbearing Radiographs After Valgus High Tibial Osteotomy for Medial Knee Arthritis is not Predictable
Klaud Miller, M.D., Agnes Maddox, R.N., Sandra El-Daccache, B.S.